NETWORK – Globalhealth
Information for Physicians




Faculty of AestheticMeso
Information on the Standard Protocol for Aesthetic Mesotherapy, Compounds Used and Membership
Search for doctors
If you are looking for a certified doctor, follow this link:
Search for doctors
Patient information
Attention! This page is intended for doctors!
Patients, who would like to inform themselves about the therapy, we ask to go to the patient information, where you find extensive patient-fair information:
To the patient information
Note for physicians
The information provided here is not intended to replace hands-on training in aesthetic mesotherapy. Within our advanced training courses you will receive numerous practical information which will strongly influence the results.
Topic navigation
NETWORK-AestheticMeso deals with the standardization of treatment techniques and active substances for the treatment of aesthetic indications with mesotherapy.
In 2006, a number of dedicated mesotherapists – mainly from the field of dermatology – started to develop a standardized treatment protocol for mesotherapy. At that time we could not foresee whether and how good this standardization would be and whether it would be accepted by our colleagues. The NETWORK for Mesotherapy, which has already existed interdisciplinary for many years, gave itself an organizational structure under the name NETWORK-ÄsthetikMeso with the publication of the developed standards, in order to enable a standardized training and to continue the started development.
Basics
The origins of today’s advanced treatment of aesthetic indications go back to the physician Michel Pistor, who developed the basics of mesotherapy in 1952. The key experience for him was the injection of procaine into the ear of a deaf patient, who could then hear again.
He developed the idea of injecting very small doses of active substances directly into the skin, bypassing the metabolism.
His motto was:
The principle consists in a planar introduction of substances in small doses into a defined skin depth (Meso = equal to medium dermis). The introduction of revitalizing and regenerating substances aims to increase the body’s own reparation and regeneration processes. The procedure uses local stimuli, pharmacological, vegetable, homeopathic and orthomolecular active agents, the depot effect of the skin as well as the diffusion of the substances into deeper skin and connective tissue layers.
For aesthetically working physicians, especially those with a dermatological background, it is of course interesting that the target and the infiltrating organ are identical. Therefore the danger of complications is almost negligible, because we only use very low doses – about 10 to 100 times lower than with systemic administration – if the corresponding indications for contraindications are observed.
In our work, we ourselves have concentrated on those active substances which, on the one hand, can treat the respective aesthetic indication positively and, on the other hand, have proven their effect through scientific monographs.
Within the NETWORK-AestheticsMeso we have taken a path supported by all members, which includes the following premises:
- We absolutely want all the indications we treat to be included in a statistic that provides us with information about effects, successes, failures, side effects and complications and thus for the first time collects objective figures for the indications we treat (first surveys in 2011 and 2015).
- We all work according to the same uniform treatment standards.
- We all use the same active ingredients. We are not dependent on having to sell a compound unchanged, but we can change compounds when we receive suggestions for improvement from our members. For example, we have changed our MesoHair mixture in the meantime because one of the active ingredients had to be associated with a higher allergy potential in recent publications.
Treatment protocol and indications
Injection techniques
Mesotherapy knows 2 injection techniques, which we carry out one after the other for each indication: The single shot injection, in which slightly higher amounts of active substances are injected selectively under the skin, and the nappage technique, which combines a salvo of many, closely spaced injections with a very low release of active substance. Nappage is closely related to the procedure known as Needling, which can improve the effect on the skin in addition to nappage.
We recommend the use of compressor guns as they provide the most comfortable treatment for patients. In combination with specially ground needles, which are slightly more expensive, the treatment is almost painless for the patients.
Indications
Skin maintenance and complexion improvement
The topic of prevention and preservation is becoming increasingly important in modern aesthetics. Self-confident patients educated to sustainability do not want to do something for themselves only when damage to the skin has already occurred, but they want to ensure at a younger age that the processes that cause skin aging start as late as possible. In our opinion, there is no better therapy for this indication than mesotherapy.
The previous treatment with mesotherapy has proven to be very good during surgery. The healing process of the skin after surgery can be improved and accelerated.
Skin and complexion improvement


(Combination of Mesotherapy & Needling)
Many factors play a role in the extrinsically damaged older skin: How elastic is the skin, how large are the pores, how much hyaluronan has remained in the skin, how strong is the pigment shift due to age spots are some of the most important questions that need to be answered in order to carry out a more precise diagnosis of the skin status. In addition, there is the question of smaller wrinkles that cannot be treated with fillers or botulinum toxin A. The colour of the skin also plays a not inconsiderable role for a vital appearance.
Aesthetic mesotherapy can improve some, but not all, of the aspects of skin aging described above. However, it must be clear from the outset to all practitioners and patients that a sequence of at least 5, better 8 treatment sessions is necessary to improve the skin status. It should also be clear that MesoLift, like any mesotherapeutic application at all, requires maintenance therapy to ensure long-term success.
Our preferred patients are those who can engage in this slow change in their skin status. The degree of intervention of mesotherapy is at the lower end of the spectrum, therefore no miracles can be expected from the therapy: It is very well suited for the treatment of coarse-pored skin and smokers’ skin with a greyish hue. Patients who have been in the sunbed for decades and therefore show the familiar leather-like skin can also be promised an improvement. Only very small wrinkles can achieve a partial improvement after the treatments, which can be further improved by combination with Needling. Needling has therefore been part of our standardized advanced training for some years.
Mesotherapy is also very suitable for the indications described above in combination with other procedures, such as superficial peelings (age spots), PRP (wrinkles, hair) or Needling (acne scars). The latest statistics document the treatment of 962 patients. Patient satisfaction is more than good in this multiple procedure with 48% very satisfied and 32% satisfied patients. Mixture: NWM-MesoLift
Hair loss
Originally we limited the indication to hair loss in female patients. In our opinion, this is still correct, although we have to state that more and more male patients also visit the practice. We treat androgenetic alopecia, also the Alopecia Areata shows very good results.
On the part of the NETWORK we make the following specifications:
-
- Patients should be treated with conventional medicine first. Only if conservative therapy is unsuccessful patients should be suggested to try mesotherapy.
- The beginning of hair loss should not be more than 2 years ago. The more current the situation, the higher the chance of a successful therapy.
Last year we again focused our goals better, because for this indication a graduated goal orientation is far better suited:
-
-
- The first goal is to stop the acute hair loss.
- A second goal is to strengthen and vitalize the existing hair.
- The third and of course most important goal is to initiate new hair growth.
-
Achieving the maximum goal is certainly not possible for every patient, but for many it is already enough if 1 and 2 are fulfilled.
In terms of numbers, hair loss is by far the most important indication. In the latest Meso Report 2015, a total of 12,500 patients were treated for hair loss. The significance of patient satisfaction with 58% very satisfied, 27% satisfied and only 16% dissatisfied patients is very high and has confirmed our concept.
In a further step, we are working on a combination protocol of MesoHair and PRP to further improve our results in patients who do not respond well.
Mixture: NWM-MesoHair
Mixtures of NETWORK-AestheticMeso
On the one hand, our mixtures are tailored to the respective indication with regard to the spectrum of active ingredients, on the other hand we have some active ingredients that generally have a skin-improving effect and support the activity of the tailored active ingredients as precursors or catalysts.
In conservative mesotherapy, procaine is used as a catalyst (booster). Our consideration when replacing this catalyst was to find an alternative that would have active properties in addition to catalysis. With a combination of silicon, rutin and multivitamins, we have achieved this very well.
Silicon supports blood circulation, is a good radical scavenger, and as a structural part of connective tissue it supports the reorganization of collagen and elastic fibers. Rutin is an antioxidant, has an anti-inflammatory effect and has positive effects on lipid metabolism.

In MesoLift,Centella Asiaticabecause of its stimulating properties, DMAE and non-crosslinked hyaluronic acid have been added.
The water-storing effect of hyaluronic acid is well known. We have had a very thin, easily injectable hyaluronic acid developed, which is also available as a single active ingredient, so that the dose can be adapted to the corresponding skin type.
DMAE (dimethylaminoethanol) is an interesting molecule that causes a lifting effect through increased acetylcholine secretion and additionally increases the elasticity of the dermis.
With MesoHairwe have added caffeine and increased the dose of Biotin/Vit H and Bepanthen/Vit B5. Caffeine increases the concentration of cyclic AMP and increases lipase activity. An insufficient supply of biotin leads to hair loss and regulates the sebum.
Publications
Meso Report 2015
Since 2011, NETWORK-AesthetikMeso has been sending a questionnaire to its members in order to statistically record the treatment results for our indications. For us, this is particularly important because there are no really good and comprehensive studies on mesotherapy, even if the literature initially appears different. One reason for this is that mesotherapy began as an empirical medicine and every user treated with his own recipes. On the other hand, many of the existing publications are not evidence-based. For this reason, there are quite rightly some articles that take a critical look at this lack of scientific knowledge (see list of publications).
Our goal as a network is first of all to gain a first statistical insight through a collection of patient results for our aesthetic indications. In order to make the treatment results comparable, we carry out the treatment according to standardized protocols and with the same active substances.
Of the indications offered by us, two have reached the limit of at least 900 to 1,000 patients, which is important for us. Two other indications had fewer patients and are therefore not considered further in this presentation.
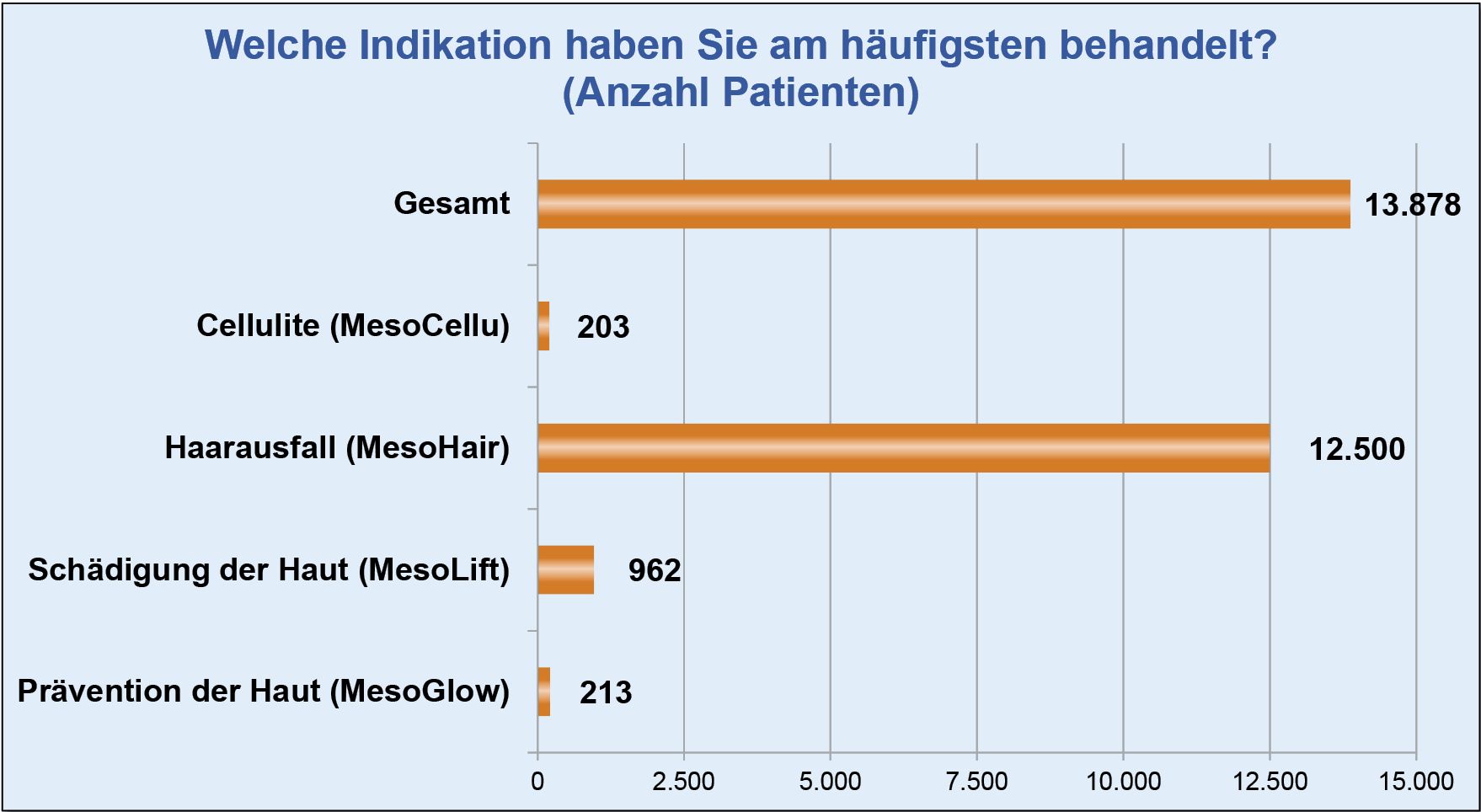
For the skin improvement with MesoLift, 962 patients were recorded in these statistics, the treatment of hair loss was performed on 12,500 patients. Both figures, especially of course the treatment of hair loss, have statistical evidence for us.
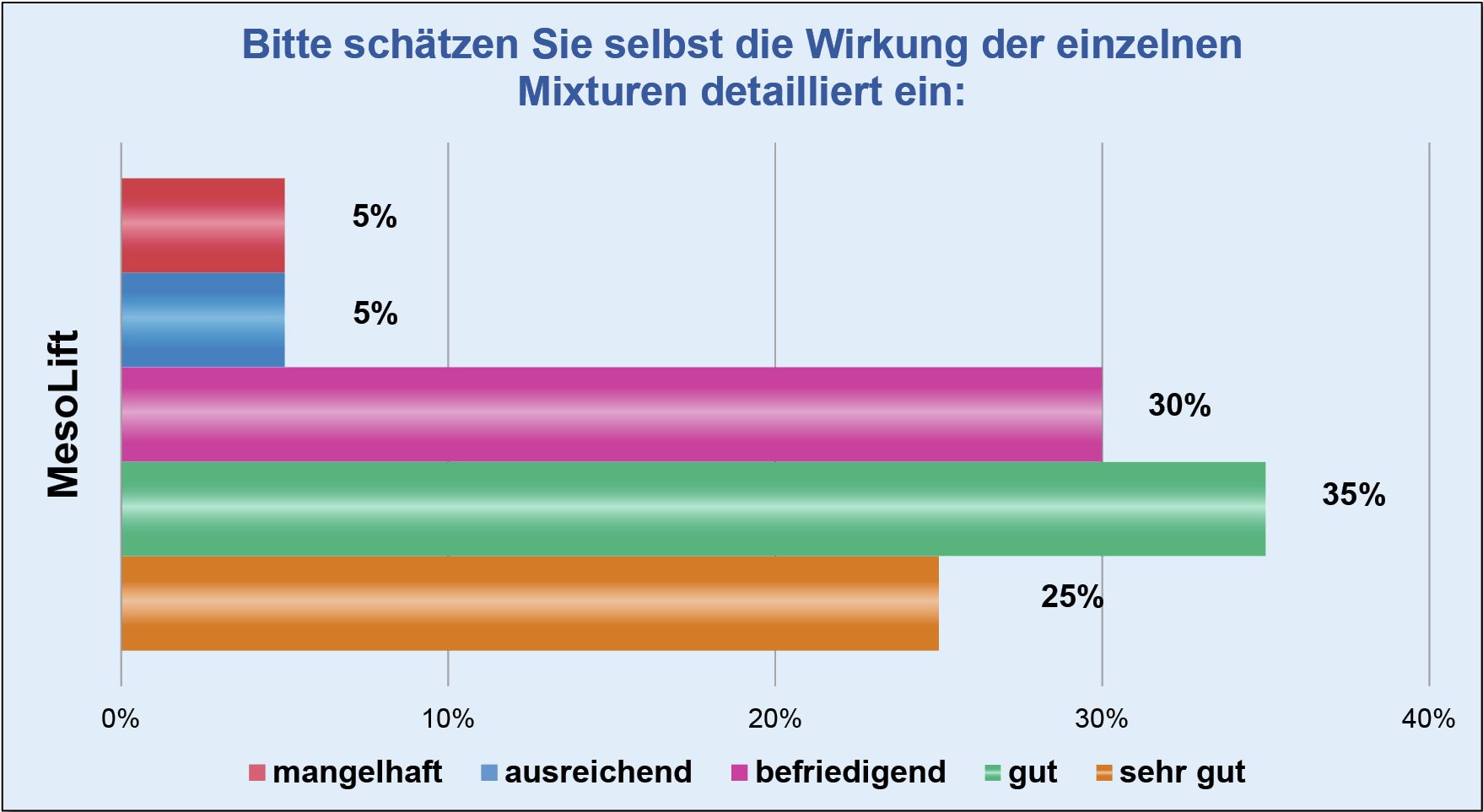
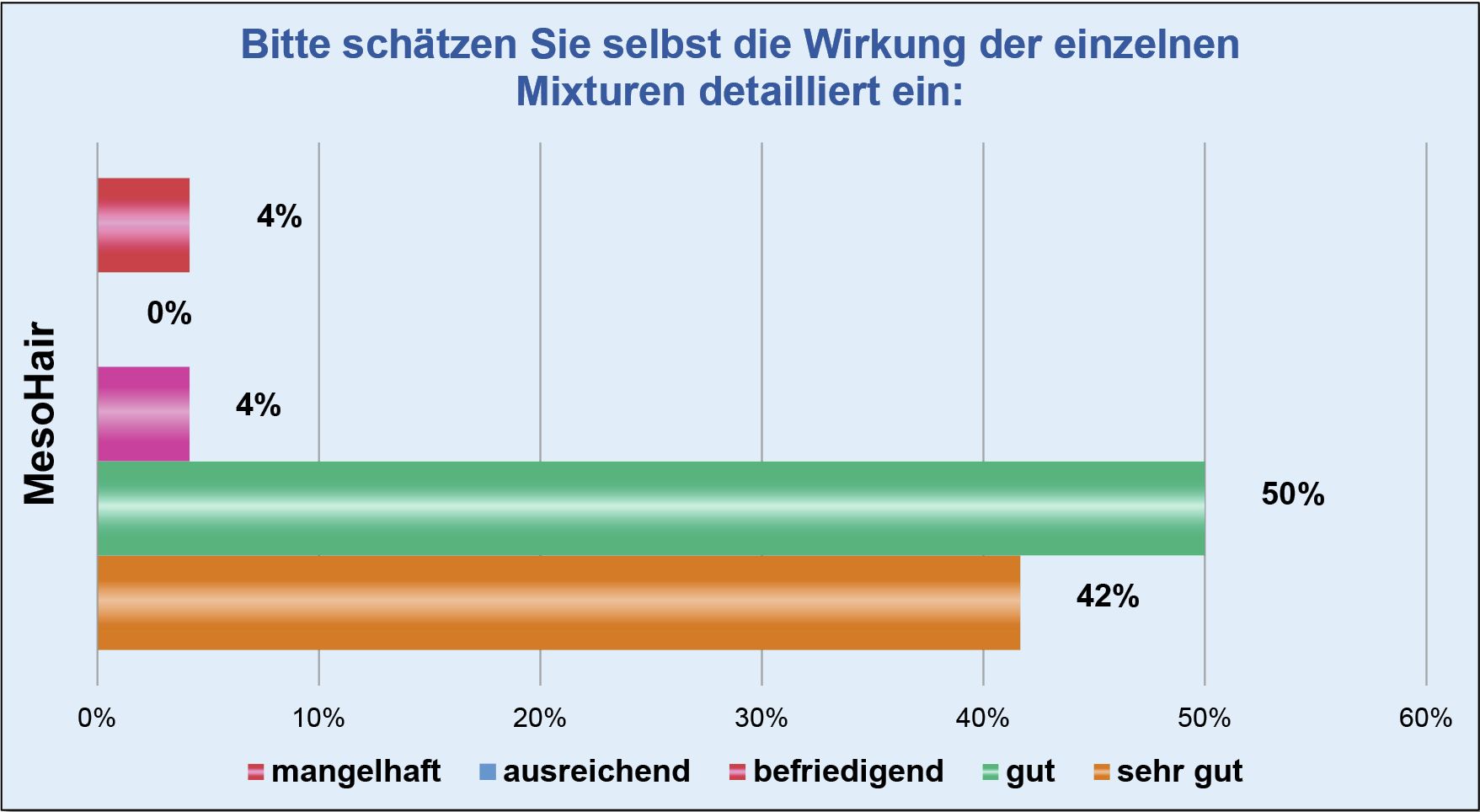
In the two diagrams above you can see how the attending physicians evaluate our mixtures. We have placed great emphasis on greater differentiation here. For us, it is no wonder that the MesoHair mixture is assessed much better. But also the values of MesoLift with 60 % good and very good as well as 30 % satisfying are quite respectable.
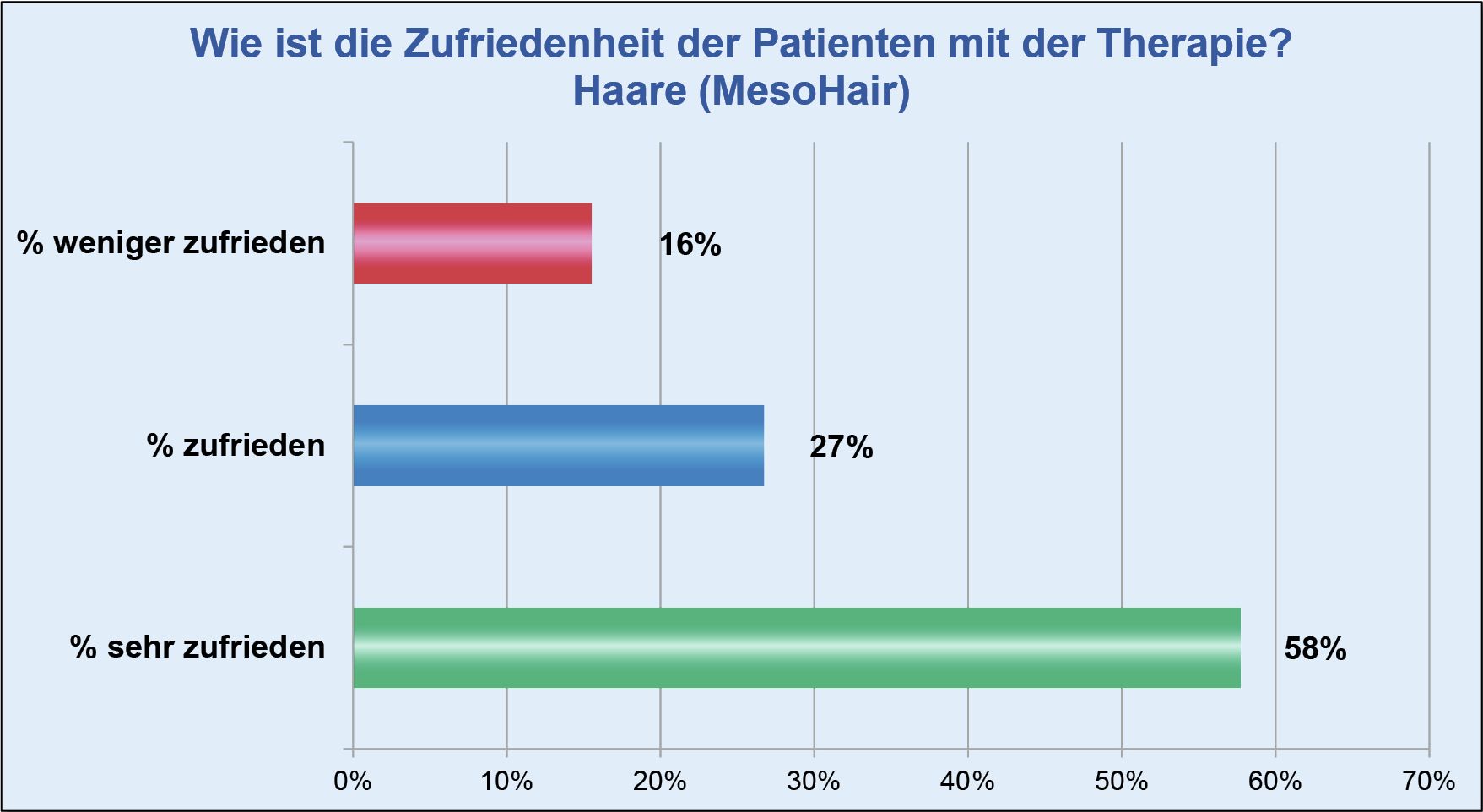
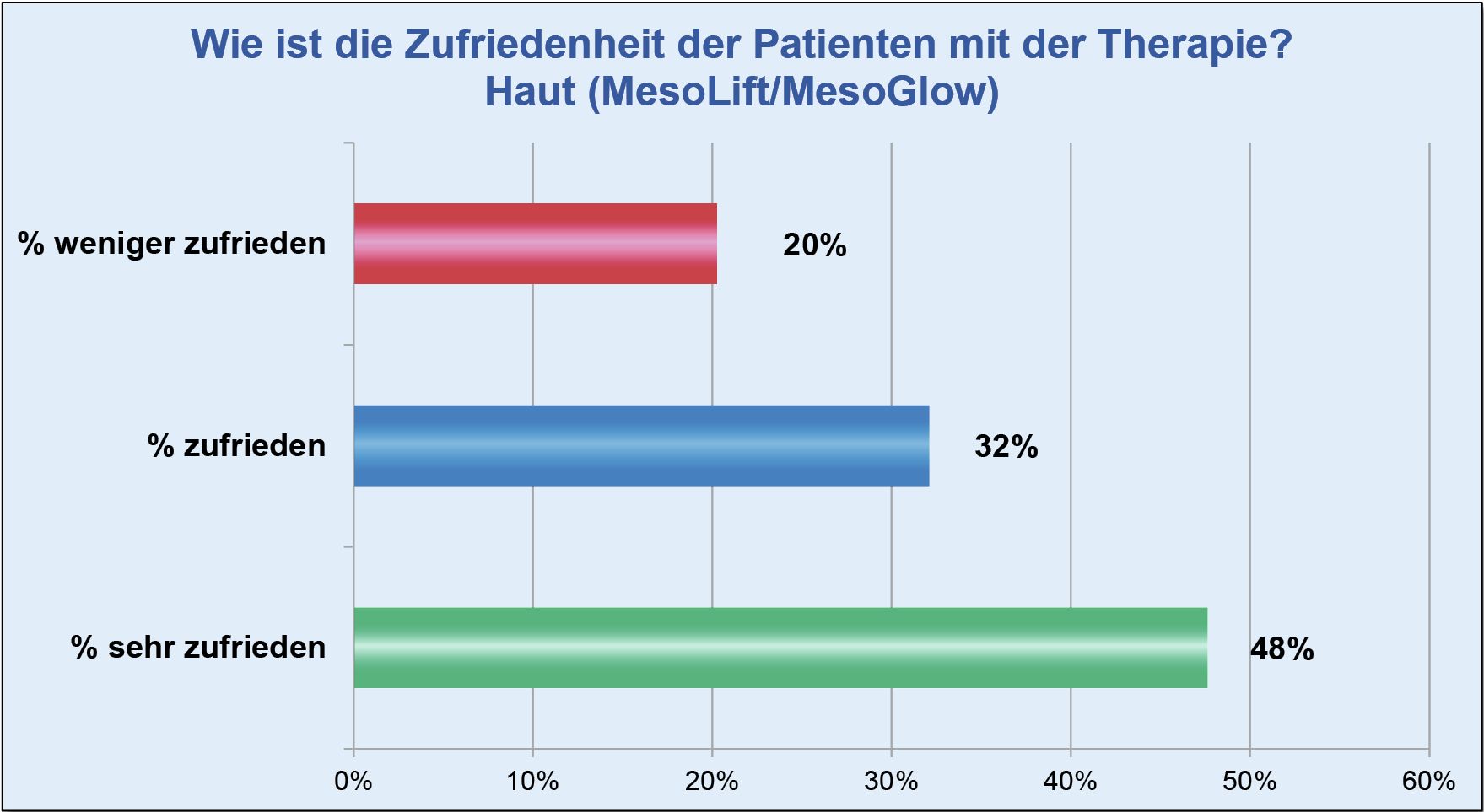
For the last two diagrams, the members interviewed their patients, with only three distinctions instead of five, to make it easier for the patients to evaluate them. 85 % satisfied and very satisfied patients show us that our members pay a lot of attention to the right patient selection.
MesoGlow/MesoLift are roughly on a par with Meso-Hair treatments in terms of patient satisfaction. The MesoLift in particular has the largest numerical share and can be used very well by us for extrinsic skin damage.
Current literature
Recommendations are marked bold
Weidmann M, Reich N: Ästhetik – Mesotherapie im Aufbruch: Neue Horizonte durch standardisierte Behandlungsprotokolle, DERM 17, 2011
Weidmann M (2012) Erste statistische Ergebnisse zur ästhetischen Mesotherapie. Kosmet Med 5(12):30–31
Weidmann M (2010) Mesotherapie heute – Entwicklung eines Behandlungsprotokolls: Versuch der Erstellung von Standards durch das NETZWERK-ÄsthetikMeso. Kosmet Med 2(10):80–83
Aust M C, Bahte S, Fernandes D: Bildatlas der perkutanen Kollageninduktion: Grundlagen, Indikationen, Anwendungen. Berlin: KVM; 2013
Weidmann M: Ästhetische Mesotherapie Heute, Spitzenforschung in der ästhetischen Dermatologie und Dermatochirurgie, 2015, 78-81
Funke G: Ästhetische Mesotherapie erfolgreich durchführen, Kosmetische Medizin 5.14, 256-257
Michael Weidmann, Martin Torzicky, Gisela Funke und Dirk Eichelberg: Alternative Methoden zur Behandlung von diffusem Effluvium und Alopecia Areata: Mesotherapie und Platelet Rich Plasma Therapie, Kosmetische Medizin 5.15, 192-194
Weidmann M (2016): 10 Jahre ästhetische Mesotherapie des NETZWERK-ÄsthetikMeso. Kosmet Med 2(16): 60-64
American Society for Dermatologic Surgery (January 2006) Technology report: mesotherapy.
Available at www.asds.net/TechnologyReportMesotherapy.aspx. Accessed 15 February 2008
American Society of Plastic Surgeons (2005) Policy statement: mesotherapy. Available at www.plasticsurgery.org. Accessed 11 February 2008
Amin S, Phelps R, Goldberg D (2006) Mesotherapy for facial skin rejuvenation: a clinical, histologic, and electron microscopic evaluation. Dermatol Surg 32(12):1467-1472
Andre P. Hyaluronic acid and ist use as a “rejuvenation” agent in cosmetic dermatology. Simin Cutan Med Surg 2004: 23: 218-222.
ASPS/PSEF (2007) Non-invasive fat-melting procedures – hype or reality? Emerging trends discussed at American Society of Plastic Surgeons Annual Meeting, October 27, 2007. Available at www.plasticsurgery.org/media/press_releases/Non-Invasive-Fat-Melting-Procedures-Hype-or-Reality.cfm. Accessed 15 February 2008
Bessis D, Guilhou JJ, Guillot B. Localized urticaria pigmentosa triggered by mesotherapy. Dermatology 2004;209:343-4.
Brandao C, Fernandes N, Mesquita N, et al. Abdominal haematoma: A mesotherapy complication. Acta Derm Venerol 85: 446, 2005.
Brown S (2006) The science of mesotherapy: chemical anarchy. Aesthetic Surg J 26:95-98
Bryant R (2004) Controversial mesotherapy: could it be the next Botox? Dermatol Times 25:1
Calikoglu E, Sorg O, Tran C, et al. UVA and UVB decrease the expression of CD44 an hyaluronate in mouse epidermis, which is counteracted by topical retinoids. Photochem Photobiol 2006: 82: 1342-1347.
Centers for Disease Control and Prevention. Outbreak of mesotherapy-associated skin reactions: District of Columbia area, January-February 2005. MMWR Morb Mortal Wkly Rep 54: 1127, 2005.
Clissold SP, Lynch S, Sorkin EM. Buflomedil: A review of ist pharmacodynamic and pharmacokinetics properties and therapeutic efficacy in peripheral and cerebral vascular disease. Drugs 33: 430, 1987
de Rigal J, Escoffer C, Querleux B, et al. Assessment of aging of the human skin by in vivo ultrasonic imaging. J Invest Dermatol 1989: 93: 621-624
Donofrio LM (2007) Mesotherapy. Cosmet Dermatol 20:97-98
Furlong W, Cunanan BA, Weymouth LA, Pearson Jl, Sockwell DC, Jenkins SR, Marr J, Tipple M, Shah DD, Blythe D, Lum GR, Glymph AC, Davies-Cole JO, Srinivasam A, Meites E, Snenshine RH (2005) Outbreak of mesotherapy-associated skin reactions – Distict of Columbia area, January-February 2005. MMWR Morb Mortal Wkly Rep 54:1127-1130
Gniadecka M, Jemec GBE. Quantitative evaluation of chronological ageing and photoageing in vivo: studies on skin echogenicity an thickness. Br J Dermatol 1998: 139: 815-821.
Gniadecka M. Effects of ageing on dermal echogenicity. Skin Res Tech 2001: 7: 204-207.
Greenway FL, Bray GA, Heber D. Topical fat reduction. Obes Res 3: 561S, 1995.
Gryskiewicz JM, Adams WP Jr (2006) Plastic surgeons rate the “hot topics”. Aesthetic Surg J 26:479-484
Hughes TA, Stentz F, Gettys T, Smith SR. Combining beta-adrenergic and peroxisome proliferator-activated receptor gamma stimulation improves lipoprotein composition in healthy moderately obese subjects. Metabolism 55: 26, 2006.
Iorizzo M, De Padova MP, Tosti A. Biorejuvenation : theory and practice. Clin Dermatol 2008: 26: 177-181.
Jemec GBE, Gniadecka M, Ulrich J. Ultrasound in dermatology. Eur J Dermatol 2000: 10: 492-497.
Kalil A (2006) Aesthetic mesotherapy: the US approach an contribution. Cosmet Dermatol 19:753-758
Kaya G, Saurat JH. Dermatoporosis: a chronic cutaneous insufficiency/fragility syndrome. Clinicopathological features, mechanisms, prevention an potential treatments. Dermatology 2007: 215: 284-294.
Kaya G, Tran C, Sorg O, et al. Hyaluronate fragments reverse skin atrophy by a CD44-dependent mechanism. PLoS Med 2006: 3: e493.
Kerscher M, Bayrhammer J, Reuther T. Rejuvenating influence of a stabilized hyaluronic acid-based gel of nonanimal origin on facial skin aging. Dermatol Surg 2008: 34: 720-726.
Lacarrubba F, Nardone B, Tedeschi A, Nordstrom R, Micali G. Ultrasound evaluation of mesotherapy for skin rejuvenation. In: Tosti A, De Padova MP, eds. Atlas of mesotherapy in skin rejuvenation. London, UK: Informa Healthcare Ltd, 2007.
Lawrence N (2003) Commentary: no smoking gun: findings from a national survey of office-based cosmetic surgery adverse event reporting. Dermatol Surg 29:1099
Lübeck RP, Berneburg M, Trelles M, et al. How best to halt and/or revert UV-induced skin ageing: strategies, facts and fiction. Exp Dermatol 2008: 17: 228-240.
Madhere S Aesthetic Mesotherapy, CRC Press,Taylor & Francis Group, © 2008 by Taylor & Francis Group, LLC, RC Press is an imprint of Taylor & Francis Group
Mesotherapy and Estetik. Available at www.mesotherapy.com/faq/. Accesses 11 February 2008
Micali G, Lacarrubba F, Tedeschi A, Nodstrom R (2008) Mesotherapy for rejuvenation of photoaged skin: Ultrasound evaluation. J Am Acad Dermatol 58:AB23
Monticone M, Barbarino A, Testi C, et al. Symptomatic efficacy of stabilizing treatment versus laser therapy for sub-acute low back pain with positive tests for sacroiliac dysfunction: A randomized clinical controlled trial with 1 year follow-up. Eura Medicophys 40: 263: 2004
Nagore E, Ramos P, Botella-Estrada R, et al. Cutaneous infection with Mycobacterium fortuitum after localized microinjections (mesotherapy) treated successfully with a triple drug regimen. Acta Derm Venereol 2001;81:291-3.
Park YY, Cellulite and Aesthetic Mesotherapy. Seoul: Hanmi Medical Publishing, 2004. P. 134.
Pistor M. [What is mesotherapy?]. Chir Dent Fr 1976;46:59-60.
Rallan D, Harland CC. Ultrasound in dermatology – basic principles and applications. Clin Exp Dermatol 2003: 28: 632-638.
Ramos-e, -Silva M, da Silva Carneiro SC. Elderly skin and its rejuvenation. Products an procedures for the aging skin. J Cosmet Dermatol 2007:6:40-50.
Rivera-Olivero IA, Guevara A, Escalona A, et al. Soft tissue infections due to non-tuberculous mycobacteria following mesotherapy: What is the price of beauty. Eferm Infecc Microbiol Clin 24: 302, 2006.
Rohrich RJ. Mesotherapy: What ist it? Does it work? Plast Reconstr Surg 115: 1425, 2005.
Rosina P, Chieregato C, Miccolis D, et al. Psoriasis and side-effects of mesotherapy. Int J Dermatol 40: 581, 2001.
Salas AP, Asaadi M. Aesthetic application of mesotherapy: A preliminary report (Abstract). Presented at the Annual Meeting of the American Society for Aesthetic Plastic Surgery, Vancouver, British Columbia, Canada, April 17, 2004.
Sandby-Moller J, Wulf HC. Ultrasonographic subepidermal low-echogenic band, dependence of age an body site. Skin Res Tech 2004: 10: 57-63.
Schmults CD, Phelps R, Goldberg DJ. Nonablative facial remodeling erythema reduction and histologic evidence of new collagen formation using a 300 micosecond 1064-nm Nd: YAG laser. Arch Dermatol 2004;140:1373-6.
Seidell JC, Bakker CJ, van der Kooy K. Imaging techniques for measuring adipose-Tissue distribution: A comparison between computed tomography an 1.5-T magnetic resonance. Am J Clin Nutr 51: 953, 1990.
Singh K (2006) Nonsurgical facial rejuvenation. J Int Med Sci Acad 19:158-164
Soncini G, Costantino C. The treatment of pathologic calcification of shoulder tendons with E.D.T.A. bisodium salt by mesotherapy. Acta Biomed Ateneo Parmense 69: 133, 1998.
Stachowski J, Botts K, Rine L, Kato D, Pollock J (2006) Mesotherapy: cosmetic applications. Int J Pharmaceut Compound 10:331-334
Tennstedt D, Lachapelle JM. Cutaneous adverse effects of mesotherapy. Ann Dermatol Venerol 124: 192, 1997.
Tokunaga K, Matsuzawa Y, Ishikawa K, et al. A novel technique for the determination of body fat by computed tomography. Int J Obes 7: 437, 1983.
Tonkovic-Capin M, Riddle CC, Schweiger ES, Aires DJ, Manson SH, Tonkovic-Capin V (2007) Brief discussion: medicolegal aspects of consent and checklists for common cosmetic procedures. Comet Dermatol 20(5):291-294
Verdier-Sévrain S, Bonté F, Gilchrest B. Biology of estrogens in skin: implications for skin aging. Exp Dermatol 2006: 15: 83-94.
Verpaele A, Strand A. Restylane SubQ, a non-animal stabilizes hyluronic acid gel for soft tissue augmentation of the mid- and lower face. Aesthet Surg J 2006: 26: 510-517.
Waller JM, Maibach HI. Age and skin structure and function, a quantitative approach (I): blood flow, thickness, and ultrasound echogenicity. Skin Res Tech 2005: 11: 221-235.
Wies L, Kerscher M. Native hyaluronic acid in dermatology – results of an expert meeting. J Dtsch Dermatol Ges 2008: 6: 176-180.